Book Appointment Now
Why Does an Erection Hurt?
When an erection hurts, the immediate psychological response is often intense anxiety. Men naturally fear permanent structural damage, loss of sexual function, or severe underlying disease. However, penile pain during engorgement is a specific mechanical symptom with a highly identifiable set of structural causes.
At Vital Wave in Woodford, our clinical team—led by Specialist Urologist Dr. Kishore Bhal alongside senior musculoskeletal and shockwave therapists Robert Shanks and Akin Celik—regularly evaluates men experiencing physical discomfort during intimacy.
Our primary objective is to separate acute structural trauma requiring immediate emergency intervention from gradual, localized inflammatory conditions that require targeted clinical management.
Is Your Penile Pain a Medical Emergency?
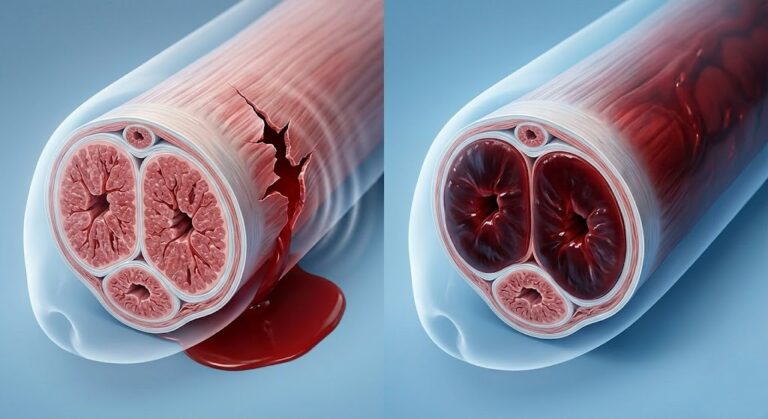
A penile plaque is not a broken bone; it is a traumatic rupture of the tunica albuginea, the tough, fibrous envelope that surrounds the erectile cylinders (corpus cavernosum).
This injury typically occurs when the erect penis is subjected to sudden, forceful bending, often during vigorous intercourse. The clinical signs are immediate and unmistakable:
An audible snapping or popping sound.
Immediate, rapid loss of the erection (detumescence).
Severe, sharp pain.
Rapid swelling and deep purple bruising across the penile shaft, caused by an intrafascial hematoma as blood escapes the ruptured cylinders.
A penile fracture is a strict medical emergency. It requires immediate surgical repair at an emergency department to evacuate the hematoma and suture the torn tunica albuginea, preventing permanent severe curvature or erectile dysfunction.
The Realities of Ischemic Priapism
Priapism is an erection lasting longer than four hours that is unrelated to sexual stimulation. Ischemic priapism occurs when arterial blood flows into the penis but the venous valves fail to open and release it.
As blood remains trapped in the corpus cavernosum, it loses oxygen, becoming acidic and toxic to the surrounding cavernous tissue. After four hours, this oxygen deprivation begins causing severe, throbbing pain.
If left untreated, the trapped blood leads to irreversible fibrosis and permanent erectile failure. Like a fracture, ischemic priapism requires immediate emergency room intervention to drain the stagnant blood and restore normal circulation.
Peyronie’s Disease & the Anatomy of a Painful Erection
If your pain developed gradually rather than from a sudden traumatic event, the most common clinical diagnosis is Peyronie’s disease. This condition is characterized by the formation of non-cancerous, fibrous scar tissue within the penis, leading to curvature and discomfort.
Microtrauma in the Tunica Albuginea: How Scar Tissue Forms
Peyronie’s disease typically originates from unrecognized microtrauma to the tunica albuginea during sexual intercourse. In a healthy healing response, the body repairs minor tissue stress efficiently. However, in men who develop Peyronie’s, the healing process becomes disorganized.
The immune system triggers an excessive localized response. Transforming growth factor-beta 1 (TGF-β1) is released, causing fibrin trapping and the rapid deposition of dense, inelastic collagen. This creates a hard, localized scar known as a fibrous plaque.
The Acute Inflammatory Phase: Why Erections Hurt Initially
Peyronie’s disease progresses in two distinct phases. The initial stage is the acute inflammatory phase, which lasts anywhere from 6 to 18 months.
During this time, the active formation of the plaque causes localized inflammation. When the penis is flaccid, patients usually feel no discomfort.
However, pain on erection occurs because the arterial blood forcibly expands the erectile cylinders, stretching the actively inflamed, inelastic scar tissue. The mechanical tension on the active lesion is what generates the sharp or aching pain during intimacy.
The Chronic Phase: When Pain Subsides but Curvature Worsens
A common source of patient confusion is the timeline of the pain. After 12 to 18 months, the active inflammation ceases. The pain from erection typically resolves completely.
However, because the fibrous plaque has stabilized into dense scar tissue, it will no longer stretch at all. As the healthy side of the penis expands with blood and the scarred side does not, the penis bends toward the plaque.
During this chronic phase, the pain is gone, but the structural curvature becomes permanent and can severely impede intercourse.

What a Fibrous Plaque Actually Feels Like
Patients often detect a plaque before they notice visible curvature. Our clinical team at Vital Wave advises men on what to look for during a tactile self-examination.
A fibrous plaque is not a superficial skin lesion; it sits beneath the skin on the rigid shaft of the penis. To the touch, it does not feel like normal, spongy tissue. Instead, it feels uniquely hard and unyielding. Patients frequently describe the sensation as feeling a “hard grain of rice,” a “rubbish pebble,” or a dense, “rubbery band” positioned along the top or side of the shaft.
Diagnostic Pathways: Looking Inside the Corpus Cavernosum
When men present at our Woodford or Chigwell clinics with painful erections or progressive curvature, Specialist Urologist Dr. Kishore Bhal relies on precise anatomical mapping to determine the extent of the vascular and structural damage.
The Role of Penile Doppler Ultrasound in Plaque Mapping
A physical examination is only the first step. To view the internal architecture of the tunica albuginea and the corpus cavernosum, we utilize a penile Doppler ultrasound.
During this procedure, a mild pharmacological agent is used to induce an erection in a controlled clinical setting. The ultrasound allows the physician to identify the exact size, density, and location of the fibrous plaques, assess the degree of curvature, and measure the arterial inflow and venous outflow of blood. This data dictates the exact medical or structural intervention required.
Reconstructive Urology: Medical and Structural Interventions
Treating curvature and the associated vascular degradation requires a highly targeted approach. Interventions range from injectable enzymes like Collagenase Clostridium Histolyticum (Xiaflex)—which directly dissolves the collagen matrix of the plaque—to mechanical remodeling via penile traction therapy.


Targeted Interventions at Vital Wave Woodford
For men dealing with the secondary effects of curvature, including vasculogenic erectile dysfunction, restoring optimal blood flow is paramount. At Vital Wave, Robert Shanks and Akin Celik utilize the world-leading EMS Swiss DolorClast system to deliver focused shockwave therapy.
This non-invasive technology sends acoustic waves deep into the erectile tissue, stimulating angiogenesis—the growth of new micro-blood vessels—and improving overall endothelial function. While acute curvature may require a multi-disciplinary urological approach, optimizing the surrounding vascular network is a core component of recovery.
If you are experiencing progressive discomfort, curvature, or an inability to maintain an erection due to mechanical tension, you can explore our complete diagnostic pathways and specialized peyronie’s disease treatment protocols. Do not ignore the early warning signs of structural damage; early clinical intervention is the most effective way to preserve long-term sexual function.